

Introduction:
Primary CNS lymphomas (PCNSL) are rare, aggressive, extra-nodal, non-Hodgkin lymphomas confined to the CNS. Other than high-dose methotrexate (MTX) based induction regimens, there are no established standards-of-care for managing PCNSL. Treatment practices across institutions vary regionally and globally. At safety-net hospitals, there are often access issues, delays in seeking medical care, and limited treatment options due to insurance barriers and other prohibitive costs. This study compares the demographics, treatment patterns, and survival outcomes among PCNSL patients treated at a safety-net hospital versus a tertiary academic institution within the same healthcare system.
Methods:
Medical records of 94 patients who were treated for PCNSL from 2007-2020, at either a public safety-net hospital (n=34) or an academic tertiary-care center (n=60), both serving the same metroplex, were analyzed. Demographics, Memorial Sloan-Kettering Cancer Center (MSKCC) prognostic class, International Extranodal Study Group (IELSG) score, induction and consolidation treatment modalities used, and survival outcomes were compared between the 2 groups. Categorical variables and response rates were compared using Fisher's exact test. Continuous variables were compared using Mann-Whitney U test. Survival functions for overall- and progression-free survival (OS and PFS) were estimated by the Kaplan-Meier method and compared using a log-rank test. Cox proportional hazards regression was used for multivariate analysis.
Results:
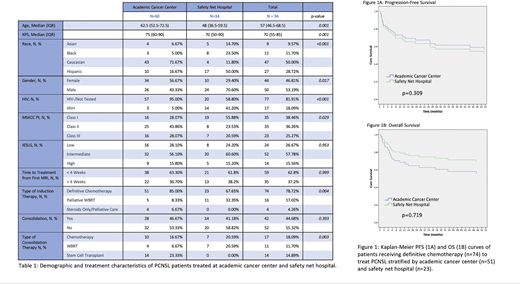
Baseline characteristics of the study population is shown in Table 1. Compared to the tertiary academic center, patients at the safety-net hospital were significantly younger, had better Karnofsky performance status (KPS) and MSKCC prognostic class, and were more commonly Black or Hispanic, male, and HIV positive. Median follow-up was 39.4 months for surviving patients and 13.1 months for all patients.
Induction regimens used were either chemotherapy (n = 74) or palliative whole brain radiation therapy (WBRT) (n = 16). Chemotherapy regimens were predominantly MTX-based (71/74, 95.9%). Safety-net patients were significantly less likely to receive induction chemotherapy (67.6% vs 85%, p = 0.004). Overall response to chemo-based induction was 70.3%. There was no significant difference in response rate to chemo-based induction between safety-net and academic center patients (73.9% vs 68.6%, p = 0.786).
Patients who had a good response to induction chemotherapy (n = 52) were either given consolidative WBRT (n =11), autologous stem cell transplant (ASCT) (n = 14), chemotherapy (n = 17), or no further treatment (n = 10). When comparing safety-net and academic center patients, hospital location did not significantly affect whether patients received consolidation therapy (82.4% vs. 80%, p = 0.735). Safety-net hospital patients were significantly less likely to receive ASCT (0% vs. 40%, p = 0.001) and had higher rates of consolidative WBRT (41.2% vs 11.4%, p = 0.03).
OS (71.7% vs. 51.1%, p = 0.218) and PFS (54.9% vs. 57.4%, p = 0.967) were not significantly different between safety-net and tertiary academic hospitals when adjusted for age and KPS. In a subset analysis, excluding patients who only received palliative care, there also were no differences in OS (68.9% vs 55.2%, p = 0.309) and PFS (50.3% vs 57.4%, p = 0.719) between hospitals (Figure 1). Patients who received consolidation treatment had significantly higher OS (84.8% vs 34.0%) and PFS (77.0% vs 30.3%), after adjusting for age and KPS (p = 0.001 for both). There were no significant differences between type of consolidation strategy employed for OS (p = 0.801) or PFS (p = 0.899).
Conclusions:
Safety-net patients with PCNSL were less likely to receive induction chemotherapy and could not receive ASCT as consolidation due to insurance barriers. Despite these differences in patterns of treatment, they had similar outcomes in terms of OS and PFS, even after adjusting for age and performance status. Consolidation treatments improved outcomes and it is critical to ensure eligible patients receive them, though the optimal type of consolidation remains unknown. This study is limited by the small sample size and retrospective analysis. Research to unearth the biologic heterogeneity of PCNSL and develop predictive biomarkers will be critical to personalize and optimize management strategies for these patients.
Awan:Genentech: Consultancy; MEI Pharma: Consultancy; Janssen: Consultancy; Astrazeneca: Consultancy; Celgene: Consultancy; Blueprint medicines: Consultancy; Sunesis: Consultancy; Karyopharm: Consultancy; Pharmacyclics: Consultancy; Gilead Sciences: Consultancy; Kite Pharma: Consultancy; Dava Oncology: Consultancy; Abbvie: Consultancy. Desai:Boston Scientific: Consultancy, Other: Trial Finding.

